A Budding Emergencist
Tuesday, November 28, 2006
Bad Day.
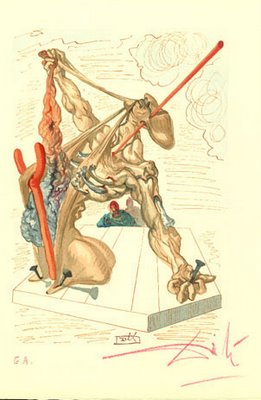
'THE FALSIFIERS', woodcut # 29 by Salvador Dalí.
This is what CHIEF RESIDENT thinks of me.
His evaluation of my first month of surgery--
FAIL.
Once more, with Feeling...
I have to repeat a month of surgery.
AND!---
Wait for it...wait for it...
He's going to evaluate my second month of surgery as well, ending in 1/5 weeks.
Guh. ¶ 1:27 AM 6 comments

'THE FALSIFIERS', woodcut # 29 by Salvador Dalí.
"Virgil now hurries Dante on to continue the journey. The poets now look into the tenth and last ditch of the Eighth Circle of Hell, and here they see the FALSIFIERS. They are punished by afflictions of every sense by darkness, stench, thirst, filth, loathsome diseases, and a shrieking din. Some of them run ravening through the pit, tearing others to pieces. Just as in life they corrupted society by their falsifications, so in death these sinners are subjected so a sum of all corruption."
This is what CHIEF RESIDENT thinks of me.
His evaluation of my first month of surgery--
FAIL.
Once more, with Feeling...
"...the falsifiers--alchemists, evil impersonators...counterfeiters, and false witnesses. These sinners, who in life, corrupted all, now are made to endure every sort of corruption and pain. Darkness, dirt, filth, disease, hunger, thirst and noise surround them."
I have to repeat a month of surgery.
AND!---
Wait for it...wait for it...
He's going to evaluate my second month of surgery as well, ending in 1/5 weeks.
Guh. ¶ 1:27 AM 6 comments
Saturday, November 25, 2006
Why My Internship Isn't a Waste

X-posted from a comment to Dinosaur's post Ancillary My Ass:
I agree with a thorough assessment before ordering any testing besides vital signs. Some points to consider with respect to testing, from the meagre experience of a lowly intern.
1. You can't make an asymptomatic patient feel better. Exception: screening--http://www.ahrq.gov/clinic/pocketgd.htm
2. In general, clinical suspicion comes before biochemistry comes before radiology comes before pathology. Example: 21 y.o. F, no PMHx, /c F/C & anorexia x 1d, 5x NBNB N/V, RLQ pain, Pelvic/guiac (-)-->Bl Cx, UCx, U/A, Chem7, LFT, GC/Chlam, RPR, PT/PTT, T&C-->EKG, CXR, XR Upright & Decubitus/Supine, CT Abdo /c IV/PO contrast, (+/-) RUQ U/S, (+/-) Pelvic U/S-->OR for tx and final pathologic dx.
3. Don't do a test unless it is going to change your management; alternatively, don't do a procedure unless you can manage the complications. Ex: Only use sedation if advanced airway management is readily available.
4. Incidentalomas are a bad thing. The more testing ordered, the greater the probability of discovering an abnormality that, once documented, must be investigated, however irrelevant to the current clinical problem. Many legal ramifications--ex: lung nodules, liver/kidney/ovarian cysts, slight anemia/hypertension/hyperglycemia/LFT abnormalities.
5. Poor communication/ history taking/ rushed sign out/ lack of PMD involvement leads to needless reinvestigation of stable chronic problems. Very common in patients with diminished capacity/ inability to communicate/ foreign-language speaking only/ lack of social support/ or with poor compliance.
Overall, for common conditions, tests should be ordered mainly to confirm clinical assessment, to rule out rare or atypical presentations, and (unfortunately) to keep the sodomites at the door. ¶ 10:12 PM 3 comments
X-posted from a comment to Dinosaur's post Ancillary My Ass:
I agree with a thorough assessment before ordering any testing besides vital signs. Some points to consider with respect to testing, from the meagre experience of a lowly intern.
1. You can't make an asymptomatic patient feel better. Exception: screening--http://www.ahrq.gov/clinic/pocketgd.htm
2. In general, clinical suspicion comes before biochemistry comes before radiology comes before pathology. Example: 21 y.o. F, no PMHx, /c F/C & anorexia x 1d, 5x NBNB N/V, RLQ pain, Pelvic/guiac (-)-->Bl Cx, UCx, U/A, Chem7, LFT, GC/Chlam, RPR, PT/PTT, T&C-->EKG, CXR, XR Upright & Decubitus/Supine, CT Abdo /c IV/PO contrast, (+/-) RUQ U/S, (+/-) Pelvic U/S-->OR for tx and final pathologic dx.
3. Don't do a test unless it is going to change your management; alternatively, don't do a procedure unless you can manage the complications. Ex: Only use sedation if advanced airway management is readily available.
4. Incidentalomas are a bad thing. The more testing ordered, the greater the probability of discovering an abnormality that, once documented, must be investigated, however irrelevant to the current clinical problem. Many legal ramifications--ex: lung nodules, liver/kidney/ovarian cysts, slight anemia/hypertension/hyperglycemia/LFT abnormalities.
5. Poor communication/ history taking/ rushed sign out/ lack of PMD involvement leads to needless reinvestigation of stable chronic problems. Very common in patients with diminished capacity/ inability to communicate/ foreign-language speaking only/ lack of social support/ or with poor compliance.
Overall, for common conditions, tests should be ordered mainly to confirm clinical assessment, to rule out rare or atypical presentations, and (unfortunately) to keep the sodomites at the door. ¶ 10:12 PM 3 comments
Friday, November 17, 2006
Surgeons as superheroes?

As I drag myself through two general surgery months in my internship, bleeding and drained, I still can not fathom the motivation that enables doctors to endure this torture. Surgery has a quasi-religious, paramilitary feel to it. With apologies to Dr. Sid Schwartz, allow me to vent.
My chief resident has me parroting this refrain: "The chief resident is always right". Even when he's wrong, he's right. For example, on evening rounds, (I had literally just begun my call, and had been away for 18 hrs, a lifetime on a surgical floor) he mentioned that a particular, delicate, demanding patient was tolerating clears. I happened (being the intern, I am expected to have all information about the patient on hand) to have the orders list in front of me. There it was, the order HE wrote that very morning, for a clear liquid diet. This is unusual in that; 1) the chief resident rarely, if ever, writes orders himself; 2) that he would forget an order he wrote; 3) would fail to take advantage of an opportunity to pimp a hapless intern in the minutiae of patient management. I, keeping above drilled maxim in front of my thoughts, refrained from correcting him. Subsequently, he reported to the attending the same, which the attending plainly denied--it was right there in the orders--"DIET: CL LIQ". I received a verbal beating for failing to correct the senior resident, and was held responsible for his embarrassment in front of the attending. This kind of pathological evasion of responsibility is beaten into the training resident from the beginning, and represents to me part of the fundamental inhumanities of surgical training.
You know, I wouldn't mind the 15 hour days, the narcissistic, entitled patients, the petty vengeful nurses, if I had some support from above. If there's no team, the whole thing falls apart.
It reminds me of a conversation I had with an attending at a different hospital who wrote me a letter of recommendation. I asked him why surgeons have to start operating at 7 or 7:30, thus needing to round at 6 AM, thus making necessary prerounding at 4:30 or 5. He said it is because the surgeon is the ultimate doctor, responsible for every facet of knowledge of medicine as well as surgical mastery. In short, surgeons must be super-heroes. While the rest of us struggle to maintain our humanity in the face of death and awesome responsibility, surgeons reach towards some ultimate, the ideal, to be the ubermensch.
Boing boing's Cory Doctorow frequently refers to comic-book superheroes as "underwear perverts," and, given the surgeon's chosen attire, I'm not sure I disagree.
My point is that, perhaps in struggling towards omnipotence ("The only way to heal is with cold steel") and omniscience (c.f. my attending's explanation), some essentially human aspects are minimized and overlooked, like compassion, responsibility, and appreciation. It's enough to be human--sometimes trying to be more than human involves denying simple humanity.
One must be human. ¶ 6:14 PM 3 comments

As I drag myself through two general surgery months in my internship, bleeding and drained, I still can not fathom the motivation that enables doctors to endure this torture. Surgery has a quasi-religious, paramilitary feel to it. With apologies to Dr. Sid Schwartz, allow me to vent.
My chief resident has me parroting this refrain: "The chief resident is always right". Even when he's wrong, he's right. For example, on evening rounds, (I had literally just begun my call, and had been away for 18 hrs, a lifetime on a surgical floor) he mentioned that a particular, delicate, demanding patient was tolerating clears. I happened (being the intern, I am expected to have all information about the patient on hand) to have the orders list in front of me. There it was, the order HE wrote that very morning, for a clear liquid diet. This is unusual in that; 1) the chief resident rarely, if ever, writes orders himself; 2) that he would forget an order he wrote; 3) would fail to take advantage of an opportunity to pimp a hapless intern in the minutiae of patient management. I, keeping above drilled maxim in front of my thoughts, refrained from correcting him. Subsequently, he reported to the attending the same, which the attending plainly denied--it was right there in the orders--"DIET: CL LIQ". I received a verbal beating for failing to correct the senior resident, and was held responsible for his embarrassment in front of the attending. This kind of pathological evasion of responsibility is beaten into the training resident from the beginning, and represents to me part of the fundamental inhumanities of surgical training.
You know, I wouldn't mind the 15 hour days, the narcissistic, entitled patients, the petty vengeful nurses, if I had some support from above. If there's no team, the whole thing falls apart.
It reminds me of a conversation I had with an attending at a different hospital who wrote me a letter of recommendation. I asked him why surgeons have to start operating at 7 or 7:30, thus needing to round at 6 AM, thus making necessary prerounding at 4:30 or 5. He said it is because the surgeon is the ultimate doctor, responsible for every facet of knowledge of medicine as well as surgical mastery. In short, surgeons must be super-heroes. While the rest of us struggle to maintain our humanity in the face of death and awesome responsibility, surgeons reach towards some ultimate, the ideal, to be the ubermensch.
Boing boing's Cory Doctorow frequently refers to comic-book superheroes as "underwear perverts," and, given the surgeon's chosen attire, I'm not sure I disagree.
My point is that, perhaps in struggling towards omnipotence ("The only way to heal is with cold steel") and omniscience (c.f. my attending's explanation), some essentially human aspects are minimized and overlooked, like compassion, responsibility, and appreciation. It's enough to be human--sometimes trying to be more than human involves denying simple humanity.
One must be human. ¶ 6:14 PM 3 comments
